MODULE 1 : Anatomy and Physiology of the Immune System
Introduction
Immunity consists of all the physiological mechanisms that allow the body to recognize materials as foreign or abnormal and to neutralize or eliminate them.
The immune system is a complex interrelationship of organs, tissues, cells and their chemical mediators. The immune system enables the body to differentiate “self” from “non-self”. The immune system is responsible for protecting against pathogens and cancer, to clean the body of dead cells, and much more while maintaining tissue integrity.
In this module, we discuss the components of the immune system and how they are able to protect the body.
Module Structure
This module contains three sections:
SECTION 1: Overview of the Immune System
SECTION 2: Cellular Components of the Immune System
SECTION 3: Vessels and Organs of the Immune System
SECTION 1: Overview of the Immune System
Learning Objectives
After reading this section, you should be able to:
- List three beneficial effects of the immune system.
- List three potentially harmful effects of the immune system.
- Define the term immunity.
- Distinguish between innate and adaptive immunity.
- Distinguish between first- and second -line nonspecific defenses.
- Distinguish between specificity, memory and tolerance of the adaptive immunity.
- Distinguish between humoral immunity and cellular immunity.
- Identify factors that alter the function of the immune system.
Functions of the Immune System
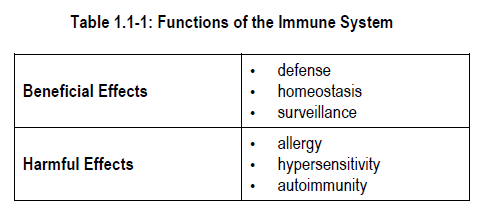
The human immune system exerts both beneficial and potentially harmful effects.
1) Beneficial effects
The beneficial effects of the immune system include:
-
-
- defense –against bacteria and viruses
- homeostasis – eliminating worn out or damaged cells from the body
- surveillance – hunts for abnormal cells that arise spontaneously and eliminates these abnormal cells or foreign materials
-
2) Harmful effects
Harm can result if the immune system is not in balance.
Allergy* and hypersensitivity* are examples of an overactive defense mechanism.
Autoimmunity results from an imbalance in the immune system’s homeostatic function. Autoimmunity occurs when immune responses are generated inappropriately against a person’s own body tissues.
When the surveillance system is imbalanced, malignancy* may result. Immune surveillance plays an important role in the prevention of malignancy. When potent drugs are used to suppress the immune system (as in transplant patients), an increase in the incidence of malignancy is seen.
Types of Immunity
Two types of immunity carry out the functions of defense, homeostasis and surveillance in the human body:
-
-
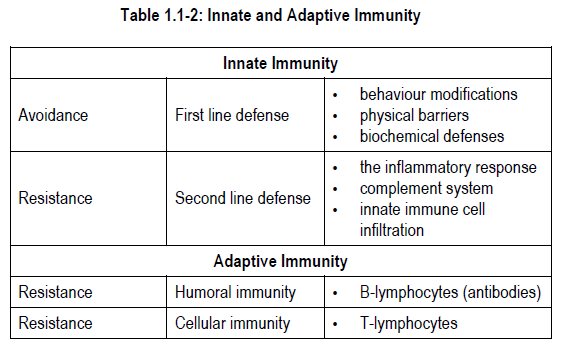
- innate immunity* (nonspecific immunity, natural immunity, genetic immunity)
- adaptive immunity* (specific immunity, acquired immunity)
-
Differences between innate and adaptive immune systems are summarized in Table 1.1-2.
Innate (Nonspecific) Immunity
Innate immunity is a permanent form of immunity with which you are born. It is present at all times in people with normal physiology. It expresses innate recognition receptors that sense the presence of factors that are classically associated to pathogens (e.g., lipopolysaccharides found on gram-negative bacteria). Therefore innate immune cells act as sensor cells and are responsible for initiating the appropriate immune response to the various forms of pathogens and microorganisms. Innate immunity is not as specific as adaptive immunity and its response will not be altered by repeated exposure to a pathogen. However, it will respond to pathogen exposure within minutes whereas adaptive immunity can take days.
Innate immunity is divided into first line and second line defenses.
1) First line defenses
First line defenses are those that prevent access of microorganisms into the human body.
Behaviour modifications and physical barriers are important first line defenses and include:
-
-
- skin
- blood-brain barrier
- mucous membranes (e.g., line the respiratory tract and urinary tract)
- tiny hairs (cilia) that expel bacteria and unwanted material from the lungs
- coughing and sneezing
- elimination of unabsorbed substances from the intestine
-
Chemical barriers also aid in preventing penetration of microorganisms. Examples of chemical barriers include:
-
-
- saliva
- mucus secreted by the mucous membranes
- acid environment of the stomach and urinary bladder
- microbiota* and enzymes in the intestines
- sweat
- lysozyme* – an enzyme found in tears, saliva, and sweat that is able to break down the cell wall of certain types of bacteria
-
2) Second line defenses
Organisms that evade the first line defenses are confronted by second line defenses of the innate immune system. Second line defenses include:
-
-
- the inflammatory response
- complement* system
- innate immune cell infiltration
-
Inflammation* is one of the most important parts of the innate immune system. The inflammatory response causes substances that combat infection to be delivered to the site of tissue injury. The inflammatory response causes vasodilation, resulting in the movement of proteins, fluid and cells from the bloodstream into an area of tissue injury.
The complement system is made up of proteins that usually circulate in the blood until they come in contact with something to which they can bind (usually something that should not be there). When this happens, a cascade of immune events is set into motion. Complement has a major role in attracting phagocytes* to an area of inflammation. Complement is also known to play a role in the body’s response against tumours.
Most importantly, during the inflammatory process, innate immune cells will migrate to the site of injury. Phagocytes will ingest microbes secrete toxic chemical mediators and cell-attracting molecules to mount the immune response.
Adaptive (Specific) Immunity
The adaptive immune system is so named because the response of the system adapts to a particular agent. In contrast to the innate system, the adaptive immune system is able to distinguish among microorganisms and can alter the intensity of its response when exposed repeatedly to the same microorganism. It can turn off the system when the invading organism has been cleared from the body. Adaptive immunity is provided by cells called lymphocytes*.
The adaptive immune system exhibits:
-
-
- specificity*
- memory*
- tolerance*
-
1) Specificity
Specificity refers to the reaction that is elicited by each specific molecular arrangement that reveals itself to the immune system. Each product of the adaptive immune system reacts only to an agent that is identical or very similar to the agent that initiated the response.
For example, a person with a specific allergy to dust would not be expected to have the same reaction if he were exposed to milk proteins.
2) Memory
Memory of the adaptive immune system means that the system learns to recognize the foreign agent and will mount an increasingly vigorous specific reaction with each exposure to that substance. For memory to occur, special cells known as memory cells must be formed.
For example, the first time a person is exposed to measles virus by immunization*, the body creates a response to the virus. It also creates a “memory” of that measles virus exposure in a memory cell. The second time the person is exposed to measles immunization, the body creates a more vigorous response to the virus (because the body remembers having seen the virus at some point in the past). This process is repeated each time a measles vaccine* is given or each time a person is naturally exposed to measles virus.
3) Immunological tolerance
Immunological tolerance, henceforth referred to as ‘tolerance’ refers to the adaptive immune system’s ability to regulate itself so that the immune response can be diminished, eliminated, and not mounted against “self” tissues.
Adaptive immunity is divided into:
-
-
- humoral immunity*
- cellular immunity*
-
1) Humoral immunity
Humoral immunity involves the production of molecules called immunoglobulins*, also called antibodies*, by activated cells called B-lymphocytes* or B cells.
Antibodies are protein molecules that are found in blood and in some external secretions. They react with specific substances called antigens*.
Antigens are any foreign substances (e.g., glycoproteins, proteins, carbohydrates, lipids) that are able to elicit a response by the adaptive immune system.
Antibodies form a major line of defense against bacteria.
2) Cellular immunity
Cellular immunity is mediated by cells called T-lymphocytes*, or T cells, that are sensitized to specific molecular structures.
Cellular immunity is involved in virtually every aspect of adaptive immunity. Although some pathologies are recognized to be mainly T-cell or B-cell mediated, a close interplay between innate immune cells, T cells, and B cells is observed in immunological processes.
Factors that Affect Immune System Functions
There are three groups of factors that influence how well the immune system can respond to foreign substances. These factors include:
-
-
- genetic factors
- physiologic factors
- environmental factors
-
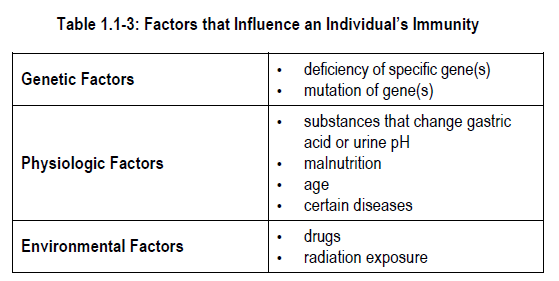
1) Genetic factors
Genes determine the way that the immune system develops in each individual. They also dictate the amount and types of immune system products (e.g., antibodies) that each individual can make. Deficiencies of specific genes translate into specific or generalized immune defects.
For example, some individuals inherit a trait for severe combined immunodeficiency syndrome (SCIDS). Individuals with this disorder are born without T-lymphocytes or B-lymphocytes. Death usually occurs within six months to one year following birth if a bone marrow transplant is not performed. We will discuss other diseases associated with genetic factors in later sections.
2) Physiologic factors
Many physiologic factors influence the function of the immune system. Substances that affect gastric acid content, alter skin or urine pH or eliminate the flushing action of tears in the eyes can increase infection in spite of an otherwise normally-functioning adaptive immune system.
Protein-calorie malnutrition accompanied by deficiencies of zinc, copper and iron is the largest contributor to altered immune responsiveness worldwide; a condition known as anergy. An individual with anergy* is identified by hyporesponsiveness to an antigen skin test, which suggests lower immune function. It needs to be distinguished from T cell anergy, a tolerance mechanism.
Age is another physiologic factor that influences the responsiveness of the immune system. Very young children and elderly adults have reduced immune responsiveness compared to individuals of other ages. As a person ages, the number and function of T-lymphocytes declines due to a process called thymic involution*. In addition, the ability to produce antibodies also declines.
Diseases that cause alterations in metabolism can influence the immune system. For example, people with diabetes have an increased risk of serious infections related to the effects of high serum glucose on white blood cell function. Other diseases associated with altered immune function include renal failure, thyroid disease and adrenal gland disorders. Many genetically determined diseases found in children are also associated with immune defects.
3) Environmental factors
Drugs are the environmental factor that influences immune responsiveness the most. Examples include:
-
-
- corticosteroids
- immunosuppressants
- biological response modifiers
- immunomodulators
-
Active immunization with vaccines also alters specific immune responses.
Radiation exposure reduces immune responsiveness. Reduced immune responsiveness is associated with extensive exposure to ultraviolet radiation in sunlight.
Location, ethnicity, and demographics also have an impact on the immune system. These factors dictate your exposure to different antigens (pollutants, food, infections) and the behaviours associated with this exposure. A striking example of that is the very low prevalence of allergic diseases in developing countries where parasitic infections are prevalent. Environmental factors coupled with genetics influence the balance between immunity and tolerance.
SUMMARY — SECTION 1: Overview of the Immune System
Cells and molecules of the immune system attempt to protect the body from foreign substances. The immune system exerts both beneficial and potentially harmful effects.
Immunity can be nonspecific (innate immunity) or specific (adaptive immunity).
Innate immunity is further subdivided into first line defenses and second line defenses. First line defenses include behaviour modifications, physical barriers and biochemical defenses. Second line defenses include the inflammatory response, innate immune cell infiltration and complement system.
The adaptive immune system is further divided into humoral immunity and cellular immunity. Humoral immunity involves the production of antibodies by B cells. Cellular immunity is mediated by T cells.
Immune responsiveness can be influenced by genetic factors, physiologic factors and environmental factors.
PROGRESS CHECK — SECTION 1: Overview of the Immune System
1.
List 3 beneficial effects of the immune system.
1) ___________________________
2) ___________________________
3) ___________________________
2.
List 3 harmful effects of the immune system.
1) _____________________________
2) _____________________________
3) _____________________________
3.
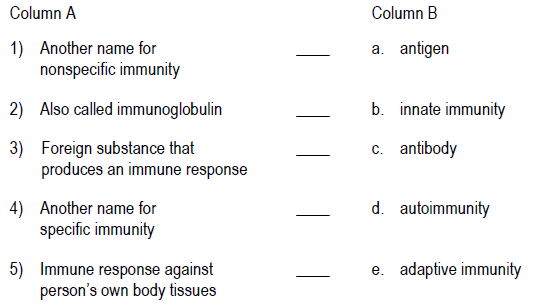
Match the definition in Column A with the correct term in Column B.
4.
Define immunity.
_____________________________
_____________________________
_____________________________
_____________________________
5.
List 4 ways that nonspecific immunity differs from specific immunity.
1) ____________________________
2) ____________________________
3) ____________________________
4) ____________________________
6.
Which of the following would be at risk for a reduced immune response?
a) a malnourished 10 year old
b) an elderly woman with diabetes
c) an anorexic teenaged girl
d) all of the above
PROGRESS CHECK ANSWERS — SECTION 1: Overview of the Immune System
1.
The immune system:
1) defends the body against pathogenic organisms
2) eliminates worn out or damaged cells from the body
3) hunts for and eliminates foreign materials or abnormal cells that arise spontaneously
2.
Activities of the immune system may cause:
1) allergy
2) hypersensitivity
3) autoimmunity
3.
1) b. innate immunity
2) c. antibody
3) a. antigen
4) e. adaptive immunity
5) d. autoimmunity
4.
Immunity consists of all the physiological mechanisms that allow the body to recognize materials as foreign or abnormal and to neutralize or eliminate them.
5.
1) You are born with nonspecific immunity, whereas you acquire specific immunity.
2) Nonspecific immunity does not require previous exposure to a microorganism; the specific immune response is based on previous exposure to microorganisms.
3) Nonspecific immunity acts fast and for a short period of time while innate immunity can last for years.
4) Nonspecific immunity does not alter the intensity of response on repeated exposure; specific immunity adapts or alters the immune response on repeated exposure.
6.
d) all of the above
SECTION 2: Cellular Components of the Immune System
Learning Objectives
After reading this section, you should be able to:
- Identify the cellular components of the innate immune system.
- State the function of each cellular component of the innate immune system.
- Identify the cellular components of the adaptive immune system.
- State the function of each cellular component of the adaptive immune system.
SECTION 2A: Cells of the Innate Immune System
Cells of the Innate Immune System
White blood cells (leukocytes) are the most numerous cells in the immune system. These cells are formed in the bone marrow from a pluripotent stem cell* (Figure 1.2-1).
The pluripotent stem cell responsible for production of all white blood cells except lymphocytes is called a common myeloid progenitor cell (CMPC).
Factors that influence growth of cells from pluripotent stem cells include:
-
-
- presence of hematopoietic* growth factors
- a suitable microenvironment in the bone marrow
-
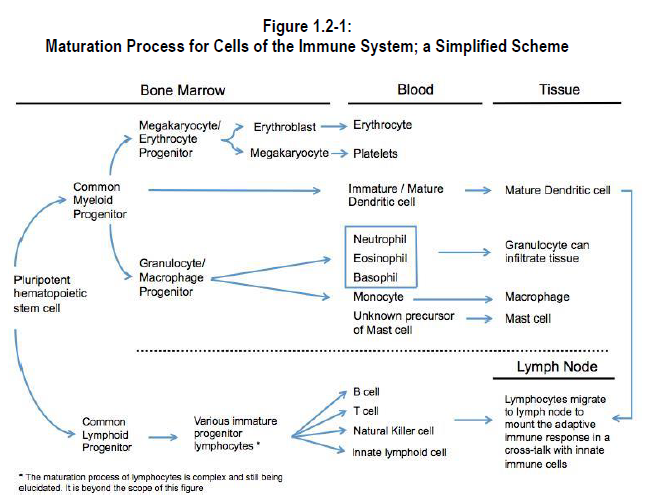
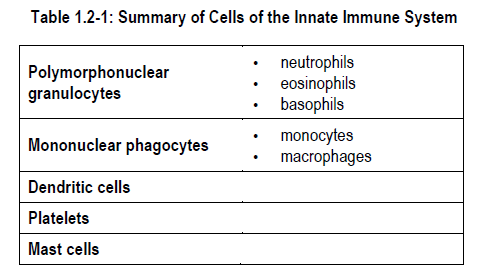
Cells of the innate immune system that are produced from CMPC include:
-
-
- the polymorphonuclear granulocytes – neutrophils*, eosinophils*, basophils*
- mononuclear phagocytes – monocytes*, macrophages , dendritic cells*
- megakaryocytes* (which produce platelets*)
-
Mast cells* also participate in innate immune reactions, but they are not produced from common myeloid progenitor. Large quantities of chemical mediators are found in the numerous cytoplasmic granules of mast cells.
The pluripotent stem cell that produces cells of the lymphoid cell line is called a common lymphoid progenitor cell (CLPC). T-lymphocytes arise from a differentiated CLPC called a pre-T cell, while B-lymphocytes arise from a differentiated CPLC called a pre-B cell. Each cell of the innate immune system will be discussed in more detail.
Polymorphonuclear Granulocytes
Polymorphonuclear granulocytes are so named because of their multi-lobulated nuclei and granular cytoplasm. The granules in each cell type stain a characteristic colour, enabling cell identification under the microscope. In addition, the granules contain substances that participate in immune reactions. The polymorphonuclear granulocytes include the neutrophils, eosinophils and basophils.
1) Neutrophils
Neutrophils comprise 60% to 70% of the white blood cells in the bloodstream.The cytoplasm of a neutrophil contains two types of granules: specific granules and azurophilic granules. Specific granules are the most plentiful.Most neutrophils are present as the mature and fully functional forms called segmented neutrophils*. If there is an urgent need for neutrophils, increased numbers of immature but still fully functional neutrophils called banded neutrophils* appear in peripheral blood.Neutrophils are short-lived cells. Their half-life in blood is approximately seven hours and they have a life span of one to four days in connective tissue. Neutrophils can survive and function normally in anaerobic conditions. For example, neutrophils remain active in poorly oxygenated tissues (e.g., necrotic tissue).
Neutrophils ingest small particles by phagocytosis. When activated by contact with a solid surface, neutrophils extend their cytoplasm to form pseudopodia*. The pseudopodia spread out and surround the foreign particle and capture it within the cytoplasm where it is then killed and digested by mediators released by the granules.
2) Eosinophils
Eosinophils are less numerous than neutrophils. They constitute only 2% to 4% of all white blood cells.
The eosinophil nucleus has two distinct lobes. Eosinophils contain only specific granules. Approximately half of the protein in the granules is a substance called major basic protein.
Although eosinophils are able to phagocytize microorganisms, they are not as efficient as neutrophils and macrophages.
Eosinophils have a longer life span than neutrophils. They are produced in the bone marrow. Once mature, they are released to the circulation, but then rapidly enter body tissues where they remain for the rest of their life (approximately 12 days).
Eosinophils can be found in the connective tissues underlying the skin, bronchi, gastrointestinal tract, uterus and vagina. It is believed that eosinophils are implicated in the defense against parasites, which are too large to be phagocytosed by macrophages and neutrophils. Along with basophils and mast cells, eosinophils are implicated in allergic reactions including in tissue damage associated with asthma.
3) Basophils
Basophils appear rarely in peripheral blood. They comprise less than 1% of circulating white blood cells.
Chemical mediators that are present in basophil granules include:
-
-
- heparin
- eosinophil chemotactic factor*
- serotonin*
- histamine
- peroxidase
-
A membrane-like material in the granules has been linked to the ability of basophils to produce prostaglandins* and leukotrienes. Prostaglandins and leukotrienes are important, especially in allergic reactions, because they can stimulate slow contraction of smooth muscles.
Basophils have actions in blood that are similar to the actions of mast cells in tissues. They function as mediator cells in inflammatory reactions. Basophils are the only source of histamine in blood. When the histamine contained in basophilic granules is released, vascular permeability is increased. Increased vascular permeability permits easier access of other immune cells to the area of local injury. Basophils display limited amoeboid movement and phagocytic activity. Basophils may, during immediate hypersensitivity reactions, migrate into selected tissues to supplement the actions of mast cells. However, basophils and mast cells are distinctly different types of cells.
Mononuclear phagocytes
Mononuclear phagocytes are named after their single nucleus and phagocytic ability. Whereas the role of the polymorphonuclear granulocytes is the secretion of toxic mediators and phagocytosis aimed at clearing pathogens, mononuclear phagocytes form the basis of the reticuloendothelial system* and are regarded as orchestrators of the immune response in tissues.
1) Monocytes
Monocytes comprise 3 to 7% of white blood cells in peripheral blood.
The half-life of monocytes in blood is 12 to 100 hours.
Monocytes represent the initial formed members of the reticuloendothelial system. They exert the same functions in the bloodstream that macrophages exert in tissue. Monocytes that cross capillary walls and enter connective tissue differentiate to become macrophages and become resident of this tissue.
2) Macrophages
In contrast to monocytes, macrophages can survive for many months in tissue. Macrophages are found in almost all tissues. Tissue-resident macrophages can arise during embryonic development or following differentiation of monocytes. They retain an ability to undergo cell division, a function that mature cells of the polymorphonuclear granulocyte family do not retain. This enables the tissue macrophage to proliferate and produce many copies of itself in local tissues. Once in tissue, macrophages respond to local tissue-specific factors (e.g., during the inflammatory process) to become specialized cells. Recently, it has been discovered that specialized macrophages can be pro- as well as anti-inflammatory, participate in tissue remodelling and much more depending on the chemical cues (i.e.chemokines) that they receive from the adaptive immune system.
The primary action of macrophages is phagocytosis and intracellular killing. Macrophages have more effective phagocytic capabilities than neutrophils, eosinophils or basophils. The canonical role of macrophages is to:
-
-
- secrete toxic chemical mediators that produce extracellular killing
- process antigens and present them to T-lymphocytes, and thus act as antigen presenting cells
- secrete chemical mediators that permit communication between the innate and adaptive immune system
-
Dendritic cells
Dendritic cells are the third class of mononuclear phagocytes and are found at the very limit between the innate and adaptive immune system. They possess long filamentous dendrites (just as nerve cells do) which they use to perform macropinocytosis* (i.e. absorb large quantities of antigens from its surrounding, a process also known as “cell drinking”). In essence, dendritic cells are professional antigen presenters involved in the maturation process of T cells.
Through macropinocytosis, they continuously sample their surrounding and, upon being activated, will migrate to the lymph node. In the lymph node they will wrap as many T cells as possible around their dendrites to select those that will proceed to the maturation step. In that regard, dendritic cells are considered as the main “sensor cells” of the immune system.
Platelets
Platelets are fragments from the cytoplasm of a giant bone marrow cell called a megakaryocyte. A platelet does not contain a nucleus; there is still a debate regarding whether or not they can be considered immune cells.
The life span of platelets ranges from 6 to 10 days.
Although most people think of platelets as being involved only in the blood clotting process, platelets also perform immune mediator functions during inflammatory reactions. Platelets release chemicals such as heparin and serotonin that:
-
-
- alter vascular permeability
- activate complement components
- attract white blood cells to the area
-
The cell surface contains a thick coat of sugars and proteins that are important for platelet adhesiveness. In addition, the platelet surface contains receptors for immunoglobulin G and immunoglobulin E, class I major histocompatibility complex products, and a receptor (arginine-glycine-asparagine) that is important for initiation of platelet-associated clotting.
Mast cells
Mast cells originate from the bone marrow stem cells, but the process of their production and maturation remains a mystery.
Mast cell granules contain histamine, neutral proteases and ECF-A (Eosinophil chemotactic factor of anaphylaxis*). The cellular constituents of mast cells enable them to manufacture and release leukotrienes with very little stimulation.
Mast cells reside in connective tissue as two distinct cell populations. The first population, called connective tissue mast cells, contain heparin in their granules. The second type, called mucosal mast cells, contain chondroitin* in their granules. Drugs that inhibit the actions of mast cells work differently on each of these two cell populations.
The surface of mast cells contains receptors for immunoglobulin E (IgE). In fact, most IgE is bound to the cell surface of basophils and mast cells; very little is found free in the bloodstream. When mast cells are stimulated to release their chemical mediators, immediate hypersensitivity reactions (e.g., anaphylaxis, anaphylactic shock*) occur.
SECTION 2B: Cells of the Adaptive Immune System
Cells of the Adaptive Immune System
The cellular foundation of the adaptive immune system is the lymphoid cell line. Lymphocytes are derived from bone marrow stem cells. Lymphocytes are relatively small cells that have a large nucleus and minimal cytoplasm.
The lymphocytes comprise 20 to 30% of all white blood cells.
Lymphocytes in peripheral blood actually represent a very heterogenous cell population. Each subpopulation of lymphocytes has a different immunologic function and a different life span. Some lymphocytes live only a few days while others survive for many months or years. Long-lived lymphocytes can even recirculate from lymph nodes* to lymph* and blood.
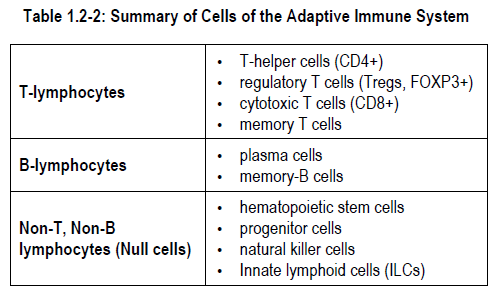
Lymphocytes of the adaptive immune system are divided into four major subsets called:
-
-
- T-lymphocytes
- B-lymphocytes
- Innate lymphoid cells (ILCs)
- Natural killer cells
-
T-lymphocytes
T-lymphocytes originate in the bone marrow but are “programmed” in the thymus* to become one of four specialized types of cells. Almost 80% of lymphocytes in blood are of the T-lymphocyte subset. T-cells localize to thymus-dependent areas of lymphoid organs (e.g., lymph nodes, spleen*). The four types of T-lymphocytes are:
-
-
- T-helper cells*
- T-regulatory cells *
- Cytotoxic T cells*
- Memory T cells*
-
The major function of T-lymphocytes is to provide cellular (cell-mediated) immunity. Cell-mediated immunity is defined as the immune effects caused by sensitized lymphocytes or activated macrophages. This type of immunity can be transferred from one individual to another only if the sensitized cells are transferred from one individual to another.
1) T-helper cells (Th cells)
The functions of T-helper cells include:
-
-
- Generally referred to as CD4+ lymphocytes (expressing the co-receptor CD4 that binds MHC-II, see Section 3). The co-receptor CD4 mainly allows recognition of antigen-presenting cells and other immune cells.
- formation of antibodies – T-helper cells produce growth and differentiation factors for B-lymphocytes
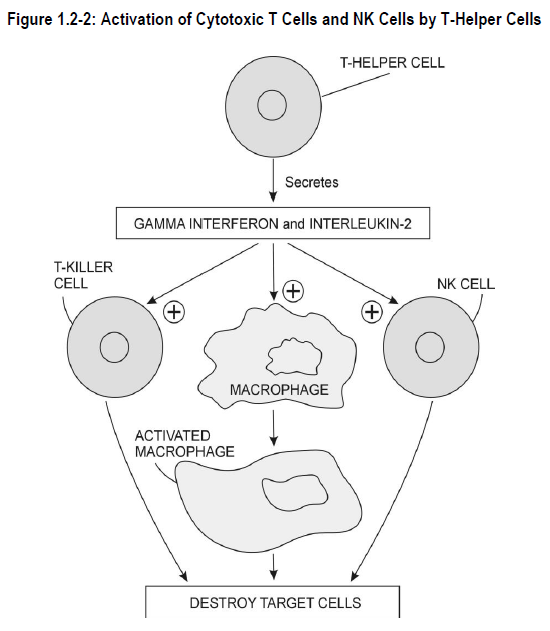
- activation of cytotoxic T cells and natural killer cells (NK)* – T-helper cells secrete the chemical mediator interferon gamma*, which stimulates the action of cytotoxic T cells and natural killer cells
- activation of inflammatory response – T-helper cells aid communication between macrophages, B-lymphocytes, bone marrow mast cells and other T-lymphocyte subsets
-
2) T-regulatory cells (Tregs)
Tregs have emerged as the major anti-inflammatory cell population of the immune system. It can be argued that their discovery has given birth to a paradox according to which immune tolerance is as important as immunity in the maintenance of a healthy immune system. The role of Tregs is to establish tolerance against self and to supress innate and adaptive immunity by:
-
-
- expressing the transcription factor FOXP3 that allows the expression of genes implicated in immune tolerance (including cytokines and various receptors; generally referred to as FOXP3+ lymphocytes)
- production of inhibitory cytokines directed against other lymphocytic populations
- direct killing or killing through metabolic disruption of T cells
- inhibition of dendritic cell maturation to dampen T cell activation and maturation
-
3) Cytotoxic T cells (T-killer cells)
Cytotoxic T cells kill specified target cells. They are generally referred to as CD8+ lymphocytes (binds MHC-I, see Section 3).
Cytotoxic T cells are T cells that directly kill other cells, not through an intermediate. Cytotoxic T cells are mainly involved in killing virus-infected cells; they are responsible for recognizing all cells of the body including non-immune cells. Cytotoxic T cells kill target cells by secreting chemical mediators and by receptor-mediated signals that instructs the target cell to go into apoptosis* and other programmed cell death pathways.
4) Memory T cells
Memory T cells are responsible for immunological memory, the process behind the long-lasting effect of vaccination. Upon recognizing a pathogen, a proportion of T cells will remain in the tissue ready for the second encounter. If the pathogen is detected by the immune system again, the cells, already present on site, will directly differentiate into effector T cells (T-helper, cytotoxic, regulatory)
Memory T cells induce inflammation associated with re-exposure to a specific molecular configuration. For example, memory T cells participate in contact allergy (skin inflammation) associated with repeated exposure to poison ivy. Other examples of memory T cell actions are the skin reactions associated with measles or a tuberculin skin test, tissue graft rejection and some nervous system conditions that follow viral infection.
B-lymphocytes
B-lymphocytes form only a small proportion (15%) of circulating lymphocytes. B-lymphocytes originate in bone marrow. B-lymphocytes differentiate to their mature subtypes within the bone marrow. B-lymphocytes localize to peripheral lymphoid tissues such as the gastrointestinal tract and the respiratory tract. Approximately 10-20% of cells in lymph nodes and 20-35% of spleen cells are B-lymphocytes.
B-lymphocytes can be classified according to cell surface markers, (i.e., to the type of immunoglobulin present on the cell surface). The immunoglobulin or antibody present on the B-cell surface is the exact one the B-lymphocyte can produce when it is stimulated by the correct antigen. The surface of a B-lymphocyte may also carry a receptor for a specific segment of antibody structure, Complement 3d or Complement 3b, or certain interleukins* or interferons*. In some cases, presence of these receptors indicates that the B-lymphocyte has become activated.
B-lymphocytes develop further when exposed to antigens in peripheral tissues. When B-cells are stimulated by an appropriate antigen, some transform to plasma cells and others transform to memory B cells* (with the assistance of T-lymphocytes).
The plasma cell produces copious quantities of antibody aimed against the specific antigen that stimulated the B-cell. The plasma cell churns out antibody for one to two days and then dies.
The memory B cell, in conjunction with the T-memory cells, enables a person to produce antibodies more quickly and in greater number the next time he is exposed to the same antigen. Memory B cells are thought to be long-lived cells.
The major function of B-lymphocytes is to provide humoral (antibody-mediated) immunity. Humoral immunity is defined as the immune effects caused by the presence of immunoglobulin antibody in blood or tissue. This type of immunity can be transferred from one individual to another only if the immunoglobulin antibody is transferred from one individual to another.
Non-T, Non-B lymphocytes
Less than 5% of circulating lymphocytes contain no markers for T-lymphocytes or B-lymphocytes. Non-B, non-T lymphocytes are sometimes called null cells because they lack the cell markers that identify T-lymphocytes and B-lymphocytes.
Non-T, non-B cells comprise a variety of cells. Null cells are thought to include:
-
-
- hematopoietic stem cells
- progenitor cells
- natural killer cells
- Innate lymphoid cells (ILCs)
-
Natural killer cells (NK) have similar functions to T-killer cells. Unlike the T-killer cells, the NK cells are not antigen-specific. The major targets of NK cells are virus-infected cells and cancer cells. NK cells bind to the target cells, then attack and kill the target cells directly.
Technique: Flow cytometry*
A technique that has revolutionized the world of immunology is flow cytometry. In a flow cytometer, a complex mixture of cell passes through a tube under a laser beam. Once the laser hits the cell, the light will be dispersed in a specific way that will be read by different light captors.
Different surface receptors and intra-cellular components can be tagged using antibodies coupled to fluorescent probes. These probes can then be read by the flow cytometer.
Therefore, a flow cytometer can be used to distinguish between lymphocytes that express, for instance, CD4, CD8, or FOXP3 within a complex cell mixture (virtually any protein can be detected if an antibody against it has been developed). This has eliminated the need for identification of the different cell populations by eye and revolutionized immunology. It has also given rise to the use of cell surface markers, or transcription factors, to refer to leukocyte and lymphocyte populations (e.g. CD4+, CD8+, FOXP3+).
SUMMARY — SECTION 2: Cellular Components of the Immune System
1) Cells of the Innate Immune System
Cells of the innate immune system are derived from a pluripotent progenitor cell in the bone marrow known as common myeloid progenitor.
Cells of the adaptive immune system include:
-
-
- polymorphonuclear granulocytes
- mononuclear phagocytes
- dendritic cells
-
Two major functions of innate immune system cells are:
-
-
- phagocytosis
- participation in inflammatory reactions
- antigen presentation
-
2) Cells of the Adaptive Immune System
Cells of the adaptive immune system include:
-
-
- T-lymphocytes
- B-lymphocytes
- non-T, non-B lymphocytes
-
T-lymphocytes are programmed in the thymus to provide cellular (cell-mediated) immunity. B-lymphocytes are programmed in the bone marrow and provide humoral (antibody-mediated) immunity.
PROGRESS CHECK — SECTION 2: Cellular Components of the Immune System
1.
Indicate which of the following are cellular components of the innate immune system or the adaptive immune system.
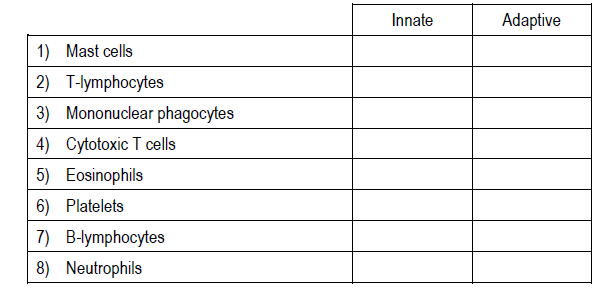
2.
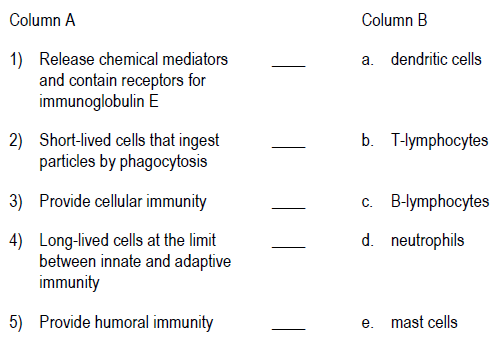
Match the function in Column A with the correct type of cells in Column B.
PROGRESS CHECK ANSWERS — SECTION 2: Cellular Components of the Immune System
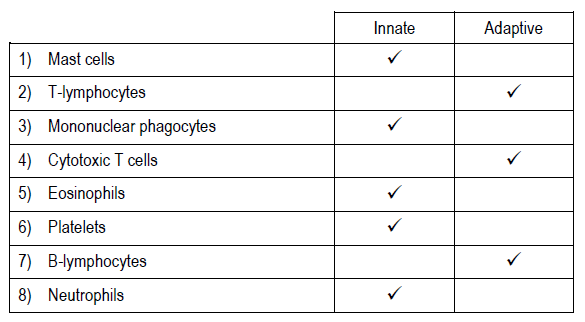
1.
2.
1) e. mast cells
2) d. neutrophils
3) b. T-lymphocytes
4) a. dendritic cells
5) c. B-lymphocytes
SECTION 3: Vessels and Organs of the Immune System
Learning Objectives
After reading this section, you should be able to:
- State the function of the lymphatic vascular system.
- Identify the primary and secondary lymphoid organs.
- Identify the function of primary and secondary lymphoid organs.
- Describe the role of intrauterine hematopoiesis in the development of lymphoid tissues.
Vessels of the Immune System
Cells of the lymphoid system circulate through the body in blood vessels of the circulatory system. The lymphatic vascular system (also called the lymphatics) drains fluid, called lymph, from the tissue spaces and returns it to the blood. The lymphatics drain almost every organ of the body. Lymphatics are not present in parts of the central nervous system, the eye, internal ear, cartilage, spleen or bone marrow.
Circulation in the lymphatic vascular system flows only in one direction – toward the heart. Fluid is forced in one direction by the contractions of skeletal muscles adjacent to small lymphatic vessels, or by smooth muscles contained within the lymphatic ducts. The lymphatic vascular system has many thin-walled channels with internal valves to prevent backflow of fluid.
Small collections of tissue called lymph nodes are interspersed along the lymphatic system. Fluid that flows along the lymphatic vascular system must pass through one or more lymph node chains before returning to the heart.
The lymphatic vascular system collects:
-
-
- lymphocytes, antibodies and other proteins from body tissues
- nutrient-rich fluid from the gastrointestinal contents
- leukocytes wandering in tissue
-
Small lymphatics eventually join together to form two large vessels called the thoracic duct* and the right lymphatic duct*.
The thoracic duct, the largest lymph vessel, draws fluid from approximately 75% of body tissues and forms the major lymphatic drainage for the gastrointestinal tract. Damage to and loss of lymph from the thoracic duct can produce abnormalities of immune function.
Organs of the Immune System
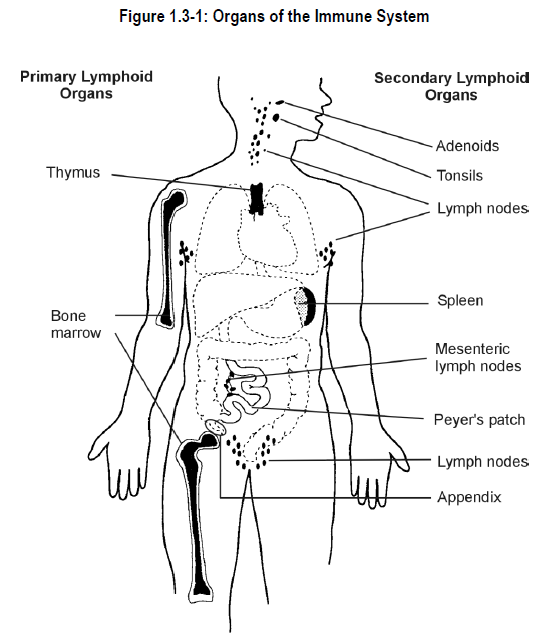
Although some cells of the adaptive immune system circulate in the bloodstream, others spend most of their time in specific body tissues or organs. Organs of the immune system are classified into two major groups (see Figure 1.3-1):
-
-
- primary lymphoid organs – sites where lymphocytes develop
- secondary lymphoid organs – sites where lymphocytes can communicate with macrophages and with other lymphocytes
-
Primary Lymphoid Organs
The primary lymphoid organs include the thymus and the bone marrow. Although both organs have been mentioned briefly, further explanation of their structure and function in the immune system is provided.
1) Thymus
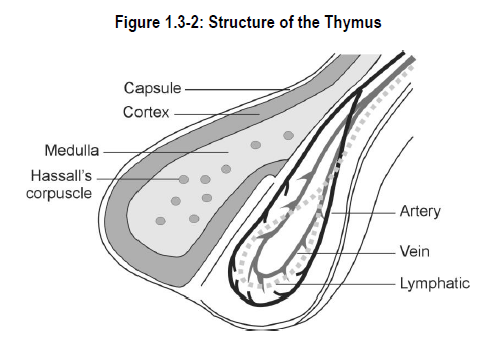
The thymus is a multilobed organ located in the chest just behind the breastbone. The thymus is capable of producing multitudes of lymphocytes, but less than 5% of all lymphocytes produced ever leave the thymus. During fetal life the thymus is colonized by lymphocytes from the blood islands of the yolk sac and hematopoietic cells in the fetal liver. Once a human is born, thymus cells originate only in the bone marrow. The thymus in elderly persons consists mostly of non-lymphoid tissue; the thymus shrinks with age in a process termed thymic involution.
The thymus is divided into the cortex (outer layer) and medulla (inner layer). The cortex is packed with small thymocytes and many proliferating T-lymphocytes (Figure 1.3-2). A complete turnover of cells in the thymus is thought to occur once every 3-4 days. The cortex contains the most immature lymphocytes. As the lymphocyte differentiates and acquires more maturity, it moves toward the thymic medulla. As the developing lymphocyte moves toward the medulla, it is challenged by regulatory systems that check to ensure the lymphocyte is able to correctly distinguish “self” from “non-self”. If the lymphocyte appears to be hostile toward body tissues, further development of that cell is suppressed. Cells that survive regulatory system challenges are eventually released into the thymic medulla, the blood or the lymphatics as mature, immunologically competent but somewhat naive T-lymphocytes. These naive T-lymphocytes move to the spleen for further education before their ultimate graduation to the general circulation, and a long life as a critical player in the adaptive immune system.
The thymic medulla contains fewer, but more mature T-lymphocytes. The medulla also contains structures, called Hassall’s corpuscles, which are of unknown function.
2) Bone Marrow
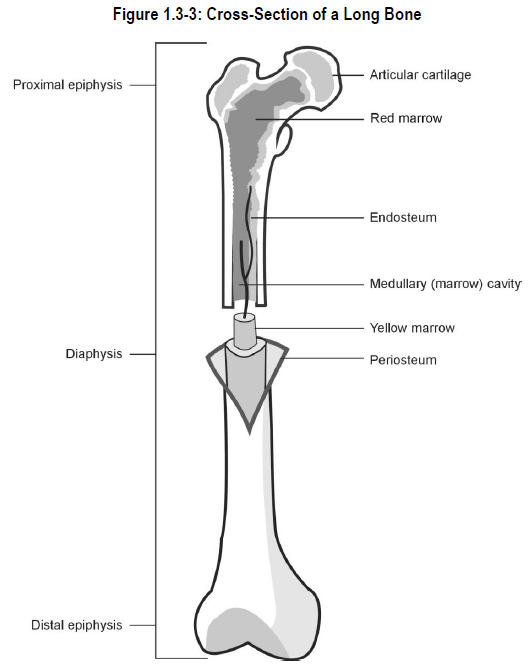
Bone marrow is contained in the spongy centre of most bones in infants and children. As bones mature, bone marrow cavities become limited to long bones (e.g., leg and arm bones), hip bones, vertebrae and breast bone of the body (see Figure 1.3-3). The bone marrow consists of vascular tissue and hematopoietic tissue.
Vascular tissue of the bone permits passage of formed blood elements between the marrow and the circulation. Most newly formed hematopoietic cells are carried to other body tissues for conditioning and testing before they are released to the general circulation.
Hematopoietic tissue is further subdivided into two types:
-
-
- red bone marrow* – forms blood cells
- yellow bone marrow* – contains fat cells that control the volume of the bone marrow cavity available for red bone marrow to grow
-
Secondary Lymphoid Organs
Secondary lymphoid organs include the lymph nodes, mucosal-associated lymphoid tissues (MALT)* and the spleen.
1) Lymph nodes
Lymph nodes are small, kidney-shaped or rounded organs made of supportive tissues that house lymphoid cells (see Figure 1.3-4). Each lymph node has lymphatic vessels entering on one side (afferent lymphatics) and exiting on the other side (efferent lymphatics). Lymph percolates through the lymph node in only one direction. By this process, lymph is filtered before it is returned to the thoracic or right lymphatic duct, and then to the bloodstream.
An important feature of lymph node structure is the lymph node sinus*. Dendritic cells and macrophages ingest foreign particles in tissues and in lymph as it flows slowly to and through the lymph node sinuses. The lymph node is the final destination of these two cell types.
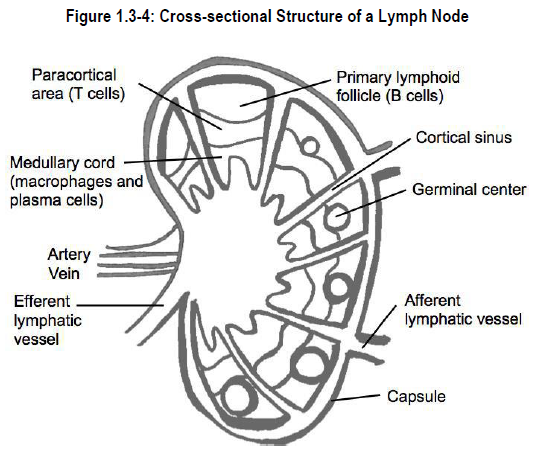
Approximately 1% of lymph actually penetrates the tissue contained within the lymph node. Lymph node tissue is divided into three regions:
-
-
- cortical region – contains predominantly B-lymphocytes
- paracortical region – contains T-lymphocytes and antigen-presenting cells (APC). APCs capture antigen on their surface and “present” it to B-lymphocytes and T-lymphocytes so that an appropriate immune response can be generated
- medullary zone – contains plasma cells
-
If lymph with retained antigen passes beyond the cortical region to the antigen-presenting cells, and if the B-lymphocyte recognizes the antigen “presented” by the APC (sometimes the assistance of T-lymphocytes is required), the B-lymphocyte may become activated.
An activated B-lymphocyte moves to an area of the cortical region called a germinal centre. Within the germinal centre the activated B-lymphocyte proliferates and gives rise to plasma cells and memory-B cells. Plasma cells migrate into the medullary zone where they manufacture antibody against the invading antigen. The antibodies and some memory-B cells are liberated into the lymph flowing through the node, and from there into the blood circulation.
With certain illnesses, lymph nodes can become enlarged due to very active development of germinal centres and plasma cells. This results in a secondary disorganization responsible for a temporary hyporesponsiveness to subsequent challenges. This is one of the reasons why vaccination programs follow strict schedules.
2) Mucosa-associated lymphatic tissue
Mucosa-associated lymphatic tissue (MALT) is lymphoid tissue that is distributed between epithelial cells within the gastrointestinal tract, the respiratory tract, the urogenital tract. Each of these body sites is a prime location for contact with substances that are “not self” and to present these substances to T and B cells. The largest collections of MALT are found in the gastrointestinal tract.
Gut MALT tissues called Peyer’s patches* contain large concentrations of B-lymphocytes and produce large amounts of immunoglobulin A (IgA) in response to antigenic stimuli from the gut lumen. Peyer’s patches also contain many T-lymphocytes that appear to reside specifically in the gastrointestinal tract.
MALT tissues are implicated in peripheral tolerance. In the case of Peyer’s patches, they are important in establishing tolerance to food and commensal bacteria. It is believed that interfering with the presentation of antigens to MALT can cause autoimmune diseases.
Other examples of local collections of lymphoid tissue include:
-
-
- the tonsils and adenoids
- mammary, lacrimary and salivary glands
- the appendix
- Waldeyer’s ring (located in the throat)
-
3) Spleen
The spleen is the largest lymphoid organ. It is found in the upper left abdomen behind the stomach. The spleen is ovoid and highly vascular. The whole of a human’s blood volume circulates through the spleen in approximately 4 minutes.
The spleen increases in size during and after digesting a meal. In cases of illness, the spleen size may exceed 9 kg in weight. A condition known as splenomegaly.
Tissues of the spleen are divided into the red pulp and the white pulp. The spleen has no connection to the lymphatics, it filters antigens from the blood.
The red pulp forms the periphery of the spleen and consists of blood vessels and blood. The transition between the artery that carries blood into the spleen and the vein that carries blood out of the spleen consists of a huge filtration bed. The filtration bed:
-
-
- stores most of the body’s platelets and granulocytes
- recycles imperfect red blood cells
- clears erythrocytes, monocyte-macrophages, platelets, granulocytes and lymphocytes from the blood
-
The white pulp is the lymphoid portion of the spleen. The white pulp contains lymphoid nodules plus lymphatic tissue that sheaths central arteries. Lymphatic sheaths selectively clear T-lymphocytes from the blood. Lymphoid nodules clear B-lymphocytes from the blood. Macrophages and activated B-lymphocytes are present in the marginal sinuses. A major purpose of the white pulp is to arrange meetings between T-cells or B-cells, antigens and accessory cells. Following these meetings, immunological responses are generated or the lymphocytes rejoin the circulating lymphocyte pool.
The marginal zone located between the red pulp and white pulp, serves as a major point for blood entry to the spleen. It consists of filtration beds. Functions of the marginal zone include:
-
-
- destruction or modification of damaged erythrocytes
- differentiation of monocytes into macrophages
- platelet storage
- retention or destruction of granulocytes
- elimination of invading microorganisms
-
Lymphoid tissue of the immune system is believed to develop following a model first proposed in the 1960s. In fetal life, the yolk sac is the site for initial development of lymphoid cells. These lymphoid cells are programmed when they move through certain fetal organs. Ultimately, lymphoid cells reside in tissues and organs that develop from other types of supportive tissue cells (epithelial and mesenchymal cells). An understanding of intrauterine blood development (hematopoiesis*) is critical to the understanding of immune system development.
Intrauterine Hematopoiesis
The yolk sac is a structure that is present in the inner cell mass (mesoderm) of the human embryo at approximately nine days following conception. A portion of the yolk sac becomes the primitive intestinal tract. The other portion remains outside of the forming embryo. This extraembryonic yolk sac differentiates to form hematopoietic cells. Intrauterine hematopoiesis consists of three overlapping phases:
-
-
- primordial (prehepatic) phase
- hepatosplenothymic phase
- medullolymphatic (definitive) phase
-
1) Primordial hematopoiesis
The first blood cells, called stem cells, become apparent during the third week of intrauterine life. Stem cells divide to form primitive precursors of red blood cells with a unique, primitive type of hemoglobin*. At this point, only red blood cells are present in the embryo.
2) Hepatosplenothymic hematopoiesis
Hematopoiesis takes place in the fetal liver and spleen starting in the second month of gestation. The liver produces precursor cells of granulocytes (e.g., cells that ultimately become basophils, eosinophils and neutrophils) and platelets. Lymphocytes are formed by fetal stem cell differentiation. Lymphocytes that circulate to the thymus mature in the thymus to become T-lymphocytes (thymocytes). Toward the end of this phase, some of the mature T-lymphocytes migrate from the thymus to populate areas of the spleen, lymph nodes and other lymphoid organs. Lymphocyte production within the spleen increases as birth becomes imminent.
The development of B-lymphocytes also occurs during this phase, however the actual site of B-lymphocyte maturation in the human fetus is uncertain. It is thought that B-lymphocytes arise from bone marrow stem cells that migrate to the fetal liver, or that they arise directly from stem cells present in fetal liver. It is also possible that the fetal bone marrow is an important site of B-lymphocyte maturation. After B-lymphocytes develop, they migrate to lymph nodes, spleen and gastrointestinal lymphoid tissue.
The non-T, non-B lymphocytes (null cells, natural killer cells), arise from bone marrow. The source of their precursors in fetal life, and the mechanism by which they become mature is not known.
3) Medullolymphatic hematopoiesis
Hematopoietic tissue begins to function within bony structures between the second and third month of gestation. The first bone to show blood-forming activity is the collarbone (clavicle). Bone marrow hematopoiesis is significant by the fourth month of gestation. Lymph nodes become very active producers of lymphocytes. Lymph nodes can even produce red blood cells just prior to birth. After birth, under normal circumstances, the bone marrow is the primary blood-forming organ. Disease conditions that produce bone marrow injury or destruction, or cancers associated with the hematopoietic system may cause the liver and spleen to resume their hematopoietic functions (extramedullary hematopoiesis).
SUMMARY — SECTION 3: Vessels and Organs of the Immune System
The immune system includes:
-
-
- lymphatic vessels
- primary lymphoid organs
- secondary lymphoid organs
-
The primary lymphoid organs include:
-
-
- thymus – site of T-cell development
- bone marrow – produces granulocytes, lymphocytes and platelets from pluripotent progenitor cells
-
The secondary lymphoid organs include:
-
-
- lymph nodes – filter fluid from the lymphatics and contain both T-cells and B-cells that respond to antigens present in lymph
- mucosa-associated lymphoid tissues (MALT) – respond to antigenic stimuli from substances that are present in the intestines, lungs and genitourinary tract and contain both T-cells and B-cells
- spleen – filters the blood and contains cells that respond immunologically to antigenic substances present in blood
-
Intrauterine hematopoiesis plays an important role in the development of the immune system. Intrauterine hematopoiesis consists of three overlapping phases:
-
-
- primordial phase – production of a primitive type of red blood cells from precursor cells called stem cells
- hepatosplenothymic hematopoiesis – production of granulocytes, platelets and lymphocytes in the liver, spleen and thymus
- medullolymphatic hematopoiesis – formation of red blood cells, white blood cells and platelets by the lymph nodes and bone marrow
-
PROGRESS CHECK — SECTION 3: Vessels and Organs of the Immune System
1.
State the function of the lymphatic vascular system.
____________________________
____________________________
____________________________
____________________________
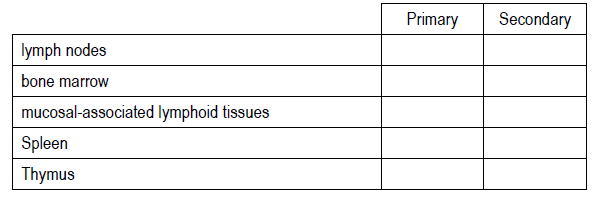
2.
Indicate whether the following organs are primary lymphoid organs or secondary lymphoid organs.
3.
Match the function in Column A with the correct lymphatic organ in Column B.
4.
Match the activity in Column A with the correct phase of intrauterine hematopoiesis in Column B.
PROGRESS CHECK ANSWERS — SECTION 3: Vessels and Organs of the Immune System
1.
The lymphatic vascular system drains lymph from the tissue spaces and returns it to the blood. Lymph contains fluid, lymphocytes, antibodies and other proteins, and leukocytes.
2.
3.
1) b. bone marrow
2) d. MALT
3) a. thymus
4) e. spleen
5) c. lymph node
4.
1) c medullolymphatic phase
2) a primordial phase
3) b hepatosplenothymic phase
MODULE 1 TEST
1.
Humoral immunity is:
a) the first line of defence of the innate immune system
b) provided by antibodies produced from activated B-lymphocytes
c) provided by T-lymphocytes
d) an extremely effective method to treat cancer
2.
Which one of the following cells is a cellular mediator of adaptive immunity?
a) neutrophil
b) T-lymphocyte
c) basophil
d) erythrocyte
3.
Cells of the adaptive immune system include all of the following EXCEPT:
a) cytotoxic T-cells
b) plasma cells
c) platelets
d) null cells
4.
Of the polymorphonuclear phagocytes, which of the following cells has the least phagocytic activity?
a) basophils
b) eosinophils
c) segmented neutrophils
d) banded neutrophils
5.
Platelets are produced by:
a) cell division during phagocytosis
b) fragmentation of megakaryocyte cytoplasm
c) plasma cells
d) natural killer cells
6.
Which of the following cells comprise the largest number of circulating white blood cells?
a) T-lymphocytes
b) neutrophils
c) eosinophils
d) monocytes
7.
Which of the following cells induce inflammation associated with re-exposure to a specific molecular configuration?
a) memory T-cells
b) regulatory T-cells
c) T-helper cells
d) cytotoxic T-cells
8.
Which of the following organs is a primary lymphoid organ?
a) thymus
b) spleen
c) mucosa-associated lymphoid tissue
d) lymph node
9.
Which of the following organs stores blood?
a) lymphatic vessels
b) lymph nodes
c) spleen
d) thymus
10.
Which of the following is a function of the red pulp of the spleen?
a) clears erythrocytes from the blood
b) manufactures lymph
c) permits platelet differentiation
d) induces a lymphocyte to become a T-lymphocyte
11.
In which portion of the lymph node are antigen-presenting cells located?
a) capsule
b) medulla
c) cortex
d) paracortex
12.
Which of the following cells is found in the germinal centre of a lymph node?
a) cytotoxic T-cells
b) macrophages
c) plasma cells
d) memory T-cells
13.
During which phase of intrauterine hematopoiesis does production of immune system cells begin?
a) adaptive phase
b) primordial phase
c) medullolymphatic phase
d) hepatosplenothymic phase
14.
Which of the following fetal organs houses the maturation process for T-lymphocytes?
a) thymus
b) liver
c) spleen
d) bone marrow
MODULE 1 TEST ANSWERS
1.
b) provided by antibodies produced from activated B-lymphocytes
2.
b) T-lymphocyte
3.
c) platelets
4.
a) basophils
5.
b) fragmentation of megakaryocyte cytoplasm
6.
b) neutrophils
7.
a) T-memory cells
8.
a) thymus
9.
c) spleen
10.
a) clears erythrocytes from the blood
11.
d) paracortex
12.
c) plasma cells
13.
d) hepatosplenothymic phase
14.
a) thymus